What is Benign Paroxysmal Positional Vertigo (BPPV)?
Benign Paroxysmal Positional Vertigo (BPPV) is one of the most common causes of vertigo:
Benign – not life-threatening
Paroxysmal – can come on suddenly and randomly
Positional – triggered by certain head positions or movements
Vertigo – a sense of rotational movement in the environment
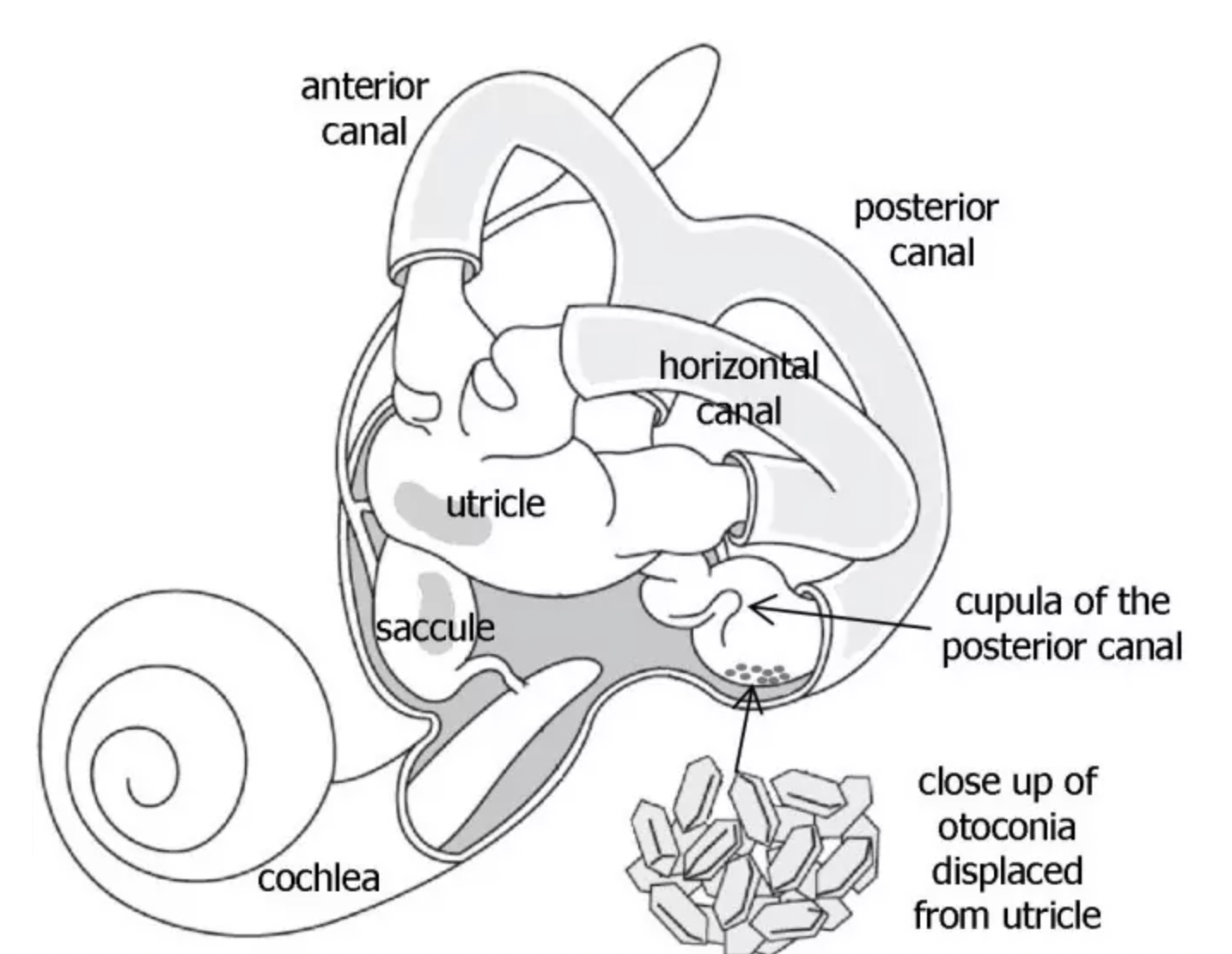
BPPV is a mechanical problem that occurs in the inner ear. It involves the otoconia, which are calcium carbonate crystals, that are normally fixed in place within the gel of the utricle. The otoconia become dislodged and move into one of the semicircular canals (for example, the posterior canal, as pictured above). There are 3 semicircular canals in each inner ear and they each respond to specific head positions. When enough otoconia become displaced in a particular canal, the movement of the fluid within that canal changes and sends abnormal signals to the brain when the head moves into the orientation of the canal.
Normally the fluid within the semicircular canals does not move; however, with BPPV, when otoconia become dislodged and move within the fluid, the nerve endings in the canal send a signal to the brain that the head is moving, even though it may not be. Since these abnormal signals do not coincide with what the other sensory organs are sensing, the conflict in sensory information results in the sensation of vertigo.
The main symptom that results from BPPV is vertigo, and the vertigo that is experienced is affected by specific head positions and movements. BPPV does not cause constant dizziness, change in hearing, headaches, or neurological symptoms. Medication is often prescribed to alleviate vertigo, but it will not address the underlying cause of vertigo. Common movements that trigger vertigo can be rolling over in bed, getting in and out of bed, looking up, bending over, and quick head movements.
Diagnosing BPPV
The defining characteristic that allows a trained vestibular therapist to diagnose BPPV is the nystagmus that results from moving the head in a particular position. Nystagmus is a very specific, involuntary, rapid, and repetitive eye movement that is triggered when the head is moved into a position that dislodges the otoconia within a specific semicircular canal. The abnormal signal that is sent to the brain causes the eyes to move in a particular nystagmus pattern, which allows the trained vestibular therapist to determine on which side and in which canal the otoconia have become dislodged. The nystagmus may or may not coincide with the sensation of vertigo.
The tests that assess for BPPV include the Dix-Hallpike and Roll Tests. It involves moving the head into a specific position and watching the eyes for a particular pattern of nystagmus. Infrared video goggles can be used to have a more clear view of the eyes in order to make an accurate diagnosis. Depending on the direction of the nystagmus, the latency of onset, and the duration of the nystagmus, a specific type of BPPV and the side in which it is occurring can be diagnosed.
Canalithiasis
BPPV canalithiasis is the type where the otoconia move freely within the fluid of the canal. The nystagmus and vertigo typically last for less than a minute, as that is how long it takes for the otoconia to stop moving once the head changes positions.
Cupulolithiasis
BPPV cupulolithiasis is the type where the otoconia have adhered to the canal. The nystagmus and vertigo typically last for longer, as the otoconia have adhered to the canal and the nystagmus and vertigo will subside once the head is moved out of the position.
Treating BPPV
Based on the defining nystagmus that results from moving the head in a particular position, a specific maneuver is performed to treat the type of BPPV that was diagnosed. The basic premise of treatment for BPPV is to take advantage of gravity to guide the otoconia back into the region where they should be, the utricle. There are a series of Canalith Repositioning Maneuvers that involve a sequence of head movements in the plane of the affected canal to try to guide the otoconia back to the utricle.
The most common maneuver is the Epley Maneuver which treats a very specific type of BPPV. Since there are multiple maneuvers and they each address a specific type of BPPV, it is important that the proper maneuver is performed in order to successfully treat the BPPV. Furthermore, it is possible to have more than one canal involved, and each would have to be addressed one at a time. BPPV treatment is very effective and can provide resolution of symptoms in 1-3 treatments. However, it may be more difficult and take longer to treat cupulolithiasis. After BPPV treatment, it is common to experience residual symptoms, such as dizziness and imbalance. It may resolve spontaneously, or require a follow-up evaluation so that Vestibular Rehabilitation exercises can be prescribed.
Can I get BPPV again?
It is common for BPPV to recur in some individuals. Although BPPV often occurs for no particular reason, it has been associated with aging, trauma, migraines, inner ear infections, viral infections, diabetes, osteoporosis, reduced blood flow, and hormonal changes. Moreover, a particular variant of BPPV can occur in one canal in the first episode and then another variant can occur in another canal in a subsequent episode. Thus, it is recommended to be assessed by a vestibular therapist for each episode to confirm the type of BPPV in order for the appropriate maneuver to be performed.
I use the Vestibular Headband from Vestibular First to show my patients the direct connection between the semicircular canals and the orientation of the head. It’s a great educational model that provides my patients with a clear understanding of the mechanics behind BPPV!
